This lecture covers the use of rib grafts in Rhinoplasty.
The rhinoplasty surgeon often encounters the need to utilize grafts when performing primary or revision surgery. Septal cartilage is typically the graft material of choice and this is especially true for primary cases. However, patients who have had prior nasal surgery or traumatic nasal collapse may lack septal cartilage or not have enough cartilage to augment and repair the nose. In these circumstances the surgeon must look to alternative sources for grafting material.

A variety of alternative grafting materials are available to the surgeon. They may be classified as autografts (from the patient’s own body), homografts (human derived grafts from a different source, ie cadaveric rib, acellular dermis), and alloplastic material. (Silastic, Mersilene, ePTFE, Medpor). The properties of an ideal structural nasal graft material include that it should be biocompatible, resistant to infection, non-resorbable, easily manipulated, structurally sound, noncarcinogenic, easy to obtain, cost-effective, and feels similar to the native nasal framework. With this in mind, the choice of grafting material should maximize the chance of long-term success and minimize the risk of morbidity.
The rib is an excellent source of grafting material. It satisfies the aforementioned criteria of an ideal graft. There is an abundant supply of cartilage in the rib, enough to achieve any surgeon’s grafting needs. The ability to harvest a long continuous portion of rib is of great benefit in select cases. This is especially helpful in cases of saddle nose deformities where longer segments of dorsal augmentation may be necessary.
In addition, both the bony and cartilaginous portion of the rib can be harvested if the surgeon prefers this. The theoretical benefit of using combination grafts of cartilage attached to bone is that it may reduce the risk of warping. Finally, rib cartilage has an inherent strength to it, especially when compared to other autografts such as ear cartilage and septal cartilage. This allows for additional nasal support that may be required to alter and maintain the nasal framework in the desired position.

This is a patient who had a revision Rhinoplasty for a saddle nose deformity, severe alar retraction, and alar collapse. Autogenous rib cartilage harvested from the medial portion of the 6th rib was used to repair his nose. This is a before and after photograph demonstrating the used of alar strut grafts and bilateral rim grafts using rib cartilage. The strength of the rib cartilage allows for marked support of the nasal ala that is persistent 1 year after correction.

As with any grafting material, the surgeon and patient must weigh the benefits and risks of the procedure. There are several potential disadvantages to using rib cartilage grafts which are discussed with the patient prior to the procedure.
Donor site morbidity is often a concern. Depending on the site of harvest, there is a potential risk of pneumothorax when dissecting over the parietal pleura. This risk is minimized with careful dissection and a leak test is performed at the conclusion of the procedure. If violation of the pleura is detected, suture repair to seal the leak is performed.
An additional donor site concern is that of scarring at the harvest site. This must be discussed with the patient prior to the procedure. Depending on the location of the harvest, the incisions can be concealed; however, the patients must be counseled regarding this prior to surgery.
Other concerns are that of pain and discomfort after surgery as well as chest wall deformities. Chest was deformities are uncommon when harvesting rib for nasal purposes as a relatively small portion of rib is harvested.
There is also a risk of graft warping after grafts are carved from the harvested portion of cartilage. This risk is minimized through balanced carving of the rib grafts. Some surgeons utilize a K-wire in the central portion of long segments of rib in order to minimize the risk of warping. Placing the desired grafts into saline prior to use allows the surgeon to observe any warping prior to use of those grafts. Any portion of the graft that warps is avoided.
Compared to other graft sources, additional time is required to harvest rib cartilage and create the grafts. The surgeon must use meticulous graft design in order to help prevent the risk of warping and visibility of the grafts.
The inherent strength of rib cartilage is an advantage to using this type of graft, as mentioned in the prior slides. However, because the graft is stronger, the nose can feel firm and inflexible after surgery especially when excessive grafting is performed and/or if the grafts are secured to fixed structures of the facial skeleton.
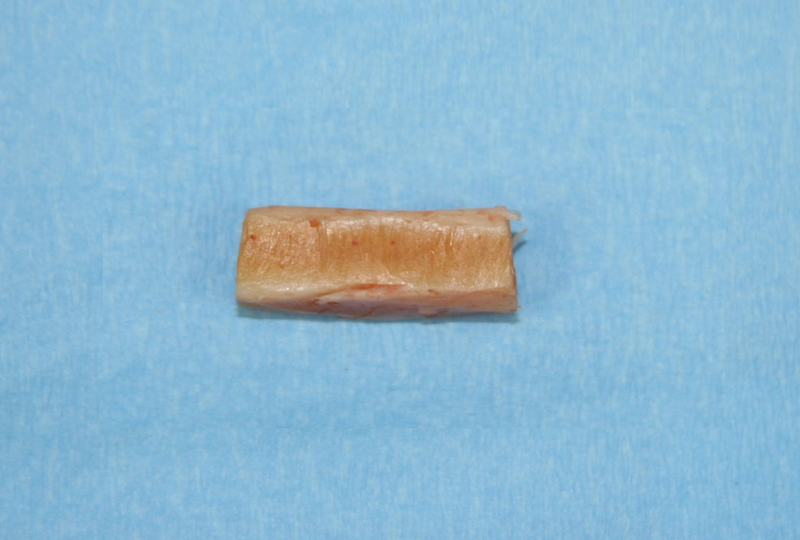
This is a portion of the 6th rib harvested from a patient for use in a revision rhinoplasty. This is the appearance of the rib cartilage prior to carving grafts. This approximately 3 cm piece has sufficient cartilage to perform bilateral spreader grafts, bilateral rim grafts, lateral crural strut grafts, and a caudal extension graft. One of the biggest benefits of rib cartilage over other autogenous grafts is the abundance of supply of cartilage. Despite this, care must be taken by the surgeon to prevent over-grafting the nose if not necessary, as this can lead to a hard, inflexible nose post-operatively.
Several factors influence the decision for the use of rib cartilage for grafting purposes. Once the goals of the rhinoplasty are established, the surgeon must determine how much grafting is necessary. If the amount of cartilage needed exceeds what is present in the septum, alternative sources are explored. Rib cartilage is selected over ear cartilage when larger and/or stronger grafts are necessary to perform the procedure.
The patient’s age also factors into the decision of performing autogenous versus irradiated cadaveric rib. Patients over 50-60 years of age tend to have increased amounts of calcification of their rib cartilage. This makes the cartilage more difficult to work with when creating grafts. In these cases, irradiated rib cartilage is considered and discussed with the patient as an alternative grafting material.

There are different approaches to rib cartilage graft harvest. I prefer harvest from the infra-mammary approach in order to harvest the 5th or 6th ribs. The benefits of this approach is that there is no need to reposition the patient for the procedure, as may be necessary when removing a portion of the floating ribs. In addition, we find that this portion of rib has less curvature to it and require less manipulation when carving your grafts.
The inframammary incision is well concealed in both men and women. The size of the incision varies based on how large a piece of cartilage is necessary, but averages approximately 4 cm. Dissection is taken down through the superior portion of the rectus muscle or the pectoralis major, depending on the level of dissection. The muscle is divided and the rib cartilage is exposed. The plane is avascular at this level and a blunt dissection is performed to expose the portion of rib to be harvested. If a longer piece of cartilage is necessary, the 6th rib can be taken along with the confluence of ribs at its medial portion. Once the rib is exposed, a 15 blade and a Freer elevator are used to elevate the perichondrium from the rib. This is preserved for grafting purposes. Next, Doyen retractors are placed to protect the underlying pleura, and a 10 blade is used to incise both the medial and lateral borders of the harvested rib. A Freer elevator is then used to free the segment of rib and remove the graft.
Once the rib segment is removed, the surgical area is filled with saline solution and several valsalva maneuvers are performed in order to rule out any leak. The incision is then closed in layers, re-approximating the muscle and then closing the dead space. The skin layer is then closed and a dressing is applied.

So now let us review some patients who have had rhinoplasty where rib cartilage was chosen as the grafting material. This first patient presented for revision rhinoplasty after having 2 previous procedures. Her last rhinoplasty was approximately 10 years ago. She had complaints about her nasal appearance as well as severe nasal obstruction.
On the lateral view you can appreciate the saddling evident in her middle vault. Her caudal septum was significantly shortened from the prior procedures as well. On her front view you can notice alar retraction and narrowing of the middle vault in the region of the saddle.

An external rhinoplasty approach was performed in order to expose the underlying nasal framework. As you can see from her intraoperative photograph, the middle vault is collapsed. In addition, there is retraction of the lower lateral cartilage with loss of support creating a concavity of her lateral crura.

Rib cartilage was harvested prior to opening the nose. An inframammary incision was made to remove the cartilaginous portion of the 5th rib. Grafts were prepared from the cartilage using balanced removal of cartilage in order to avoid warping. The cartilage was then placed in saline and allowed to soak for approximately 1 hour while the nose was dissected. Portions of cartilage that warped within the saline during this time period were discarded and only the remaining straight portions (some of which are exhibited in this photograph) were used as grafts.

In order to repair her saddle, extended spreader grafts were attached to the caudal portion of the nasal bone and the native dorsal septum. The grafts project past the native septum in order to correct the saddle. A caudal extension graft was then sutured to the anterior nasal spine and connected to the extended spreader grafts. This formed a new L-strut, repairing the saddle and lengthening the nose.

The collapsed nasal tip was repaired using sutures to repair the previous dome division. Bilateral lateral crural strut grafts were then place to support the weakened lateral crura.

Improvement in the nasal base is noted with reduced collapse of the lower lateral cartilage and support of the nasal base. This resulted in a post-operative improvement in her nasal obstruction.

This next patient presented with severe nasal obstruction and was unhappy with the appearance of her nose. She had a history orthognathic surgery with a Le-Forte 1 osteotomy. After the procedure she has nasal obstruction and a subsequent septoplasty was performed. Almost immediately after this septoplasty procedure she notes that her nose appeared collapsed and flat. She presented to me 1 year after that surgery. Upon examination of her nose she had total loss of the cartilaginous portion of the septum. This created a severe saddle nose. She also lacks support of her nasal tip.
This case required reconstruction of the entire L-strut considering the complete lack of cartilage. Rib cartilage was chosen as the grafting material due to the amount of material needed.

The cartilaginous portion of the 6th rib cartilage was harvested through an inframammary incision. In this case, a longer piece was necessary to cover the length of the nasal dorsum. Balanced carving of the rib cartilage was performed to create a dorsal graft and a coluemllar strut graft. The columellar strut was sutured to the anterior nasal spine and connected to the dorsal onlay graft that was inserted into a precise sub-periosteal pocket at the radix. The graft was thinned at this area in order to create a smooth transition along the dorsum. I should note on this view that chin augmentation was refused by the patient, though strongly recommended.
Support of the nasal dorsum and tip through creation of a new L-strut from rib cartilage graft allows for the marked improvement seen in the lateral view.


She is 1 year after surgery in these photos. She has less flattening of her nasal tip. Also notice the improvement in the projection and support of her nasal tip on the base view.